|
Research Ideas and Outcomes :
Grant Proposal
|
|
Corresponding author: Solveig E.S. Hausken (solveig.sand.hausken@gu.se), Natalie Barker-Ruchti (natalie.barker@gu.se)
Received: 21 Oct 2018 | Published: 30 Oct 2018
© 2018 Solveig Hausken, Natalie Barker-Ruchti, Astrid Schubring, Stefan Grau
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation:
Hausken S, Barker-Ruchti N, Schubring A, Grau S (2018) Injury-Free Children and Adolescents: Towards Better Practice in Swedish Football (FIT project). Research Ideas and Outcomes 4: e30729. https://doi.org/10.3897/rio.4.e30729
|
|
Abstract
This interdisciplinary research project will produce evidence-based recommendations on how injuries in Swedish youth football (soccer) can be prevented. Fewer injuries will positively impact athlete health, performance and career longevity and have the potential to promote life-long physical activity and wellbeing.
Injury pattern research demonstrates that injuries are a significant problem in (Swedish) youth sport. Football has a higher traumatic and overuse injury rate than many contact/collision sports (e.g., field hockey, basketball). In research on youth football, the incidence of overuse training injuries was measured as high as 15.4 injuries per 1000 training hours, and the incidence of traumatic and overuse match injuries was 47.5 injuries per 1000 match hours. The injury frequency is alarming and applies to the 54% of children aged 7-14 and the 39% of youths aged 15-19 years who participate in Swedish organised sports. A large body of research identifies injury risk factors and preventative strategies; however, as the recent IOC consensus statement on youth athletic development points out, the existing, mostly bio-medical knowledge does not provide effective evidence-based injury prevention strategies. To address this deficit, interdisciplinary and context-driven knowledge on injury development in youth sport is needed.
The proposed project will produce scientific evidence through four consecutive studies: a) Questionnaire to register the types, frequency and management of injuries; b) Laboratory testing of biomechanical, clinical and training-specific parameters to establish individual physical and sport-specific dispositions; c) Observation of sporting contexts to understand sporting cultures, coaching methods and coach-athlete relationships; and d) Interviews with coaches and players to recognize knowledge that shapes coaching and training. The sample of youth players will be recruited from Sweden’s most popular and injury-prone sport: football. Each of the four studies will conduct its own data production and analyses, and a collective analysis will produce integrated evidence. Concrete recommendations for best sporting practice will be developed, which will serve sporting federations, sport education institutions, coaches, sport support staff and players.
Keywords
Injury development; soccer; youth; interdisciplinary research methodology
Existing knowledge on injury risk factors in youth sport
Injury pattern research demonstrates that injuries are a significant problem in (Swedish) youth sport (
Football has a higher traumatic and overuse injury rate than many contact/collision sports (e.g., field hockey, basketball) (
A large body of literature on child and adolescent sport injury risk factors and prevention strategies exists (
Growth and maturation
Research has shown that growth and maturation is a determinant injury predictor for children and adolescents (
Biomechanical and training parameters
In terms of biomechanical, clinical and training parameters, several authors have pointed to the multidimensional nature of (overuse) injury onset
Sporting contexts and coaching practice
Sporting contexts in youth sport have been examined, although with less direct focus on injury risk factors and prevention. Nevertheless, psychological research demonstrates that a positive motivational climate is important for continued athlete participation and social development (
Norms
Research has shown that athletic ideals and norms are specific to the settings they exist in. Competitive and performance-oriented contexts are likely to involve values relating to continuous progressive performance enhancement and winning (
Key scientific gaps and shortcomings
Despite a large body of literature on sport injury risk factors and prevention strategies, Swedish children and youth sustain injuries (e.g.,
Additional scientific gaps include:
- Relationship between maturation and injury development and prevalence;
- Relationship between injury history and general health and injury development and prevalence;
- Relationship between training parameters and recovery times and injury development and prevalence;
- Relationship between injury prevention knowledge in coaches and players and injury development and prevalence.
Further, a number of methodological and conceptual shortcomings are recognized to limit injury knowledge. As mentioned above, the injury rate in football is high. However, a wide variation in injury definitions and methodologies currently creates significant differences in the results and conclusions obtained from present studies (
To address the prevalence and difficulty of detecting injuries (especially overuse injuries), the Oslo Sport Trauma Research Center (OSTRC) has developed injury registration tools that are sensitive to a greater variety of injuries and health problems. The OSTRC Overuse Injury Questionnaire registers overuse problems in sports epidemiology (
In order to address current gaps and shortcomings, the Injury-Free Children and Adolescents: Towards Better Practice in Swedish Football (FIT project) will build on latest injury research and implement the conceptual and methodological recommendations provided in studies on football injuries (
'Any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities. An injury that results in a player receiving medical attention is referred to as a ‘‘medical attention’’ injury, and an injury that results in a player being unable to take a full part in future football training or match play as a ‘‘time loss’’ injury' (Fuller et al., 2006, p. 193).
The FIT-project’s purpose and hypotheses also build on the previous mentioned research gaps and shortcomings.
Purpose and hypotheses
The overarching research purpose of the FIT-project is to provide evidence-based interdisciplinary injury prevention strategies. To achieve this, the proposed research will produce a comprehensive and integrated picture of injury etiology through investigating injury development and prevention in a sample of male and female Swedish football players aged 10 to 19.
The FIT project’s main hypothesis is that injuries develop from multi-faceted and interconnected individual, physical and contextual factors. Furthermore, the FIT-project hypothesizes that:
- Growth and maturation are potential injury risk factors for football players aged 10 to 19;
- Injury history and general health are potential injury risk factors for football players aged 10 to 19;
- Biomechanical and clinical parameters are potential injury risk factors for football players aged 10 to 19;
- Training factors, particularly training intensity and recovery time between trainings, are potential injury risk factors for football players aged 10 to 19;
- Contextual factors, especially pressure to perform, athletic ideals and coach injury prevention knowledge are potential injury risk factors for football players aged 10 to 19.
Research methodology
The FIT-project is designed as a longitudinal prospective study conducted at the Department of Food and Nutrition, and Sport Science, University of Gothenburg, Sweden. In order to capture multiple risk factors, the project combines the disciplines of biomechanics, sport medicine, sport coaching and sport sociology. As part of the interdisciplinary approach, the research methods of questionnaire, biomechanical and clinical measurements, training protocol, ethnographic observations, and semi-structured interviews will be used. The interdisciplinary and multi-methodological approach is realized through four sub-studies, which each are guided by specific research questions, but are brought together in a common analytic procedure.
Research context
The research context will be two sport schools, a football academy, and a physiotherapy and rehabilitation clinic, which are all located in a large sport and hotel complex. The research team will collaborate with the schools' principals and teachers, the footall academy's administrators and coaches, and the clinic's manager and a number of physiotherapists. The two schools are a primary and upper secondary school for children aged 10 to 15 and a high-school for pupils aged 16 to 19. In total, the two schools educate 499 pupils (n=324 for upper secondary school; n=175 for high school). Both schools are standard Swedish day schools, which provide pupils with breakfast after morning training and a cooked lunch meal, and access to a nurse.
Sample criteria
The sample criteria for players and coaches differ between sub-studies 1, 2, and 3 and 4. For sub-study 1, the inclusion criterion for players is to attend either of the two participating football schools (primary - 10-12 years; upper secondary - 13-15 years; high school levels - 16-19 years). For sub-study 2, the player inclusion criteria are being (a) injury-free and healthy at the outset of this sub-study; and (b) a player at the participating football schools, football academy, or, as the academy does not train female high-school players, players that practice football at other clubs/academies. The coach inclusion criterion is to be a coach at the participating football schools or academy. For sub-studies 3 and 4, we will choose extreme cases of male and female player's with no or multiple injuries based on data from sub-studies 1 and 2. As much as possible, the selected male and female players will represent the different age groups.
Recruitment
The recruitment of players and coaches follows a tunnel procedure (Fig.
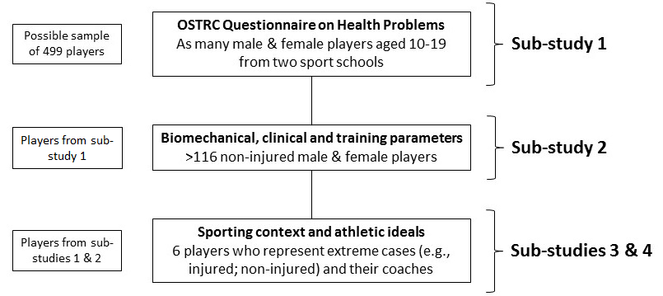
- Sub-study 1: all pupils attending the two collaborating football schools (possible sample is 499 players);
- Sub-study 2: only non-injured and healthy players (n≥116) from sub-study 1 attending the sport schools (plus female high-school players from their respective club or other academies), equally split by gender and the age groups;
- Sub-study 3 and 4: six players who all have participated in sub-studies 1 and 2, as well as their coaches.
Recruitment of players will be as follows: First, documentation consisting of project information, ethical safeguarding and consent forms for children and adolescents and parents/guardians will be handed out to the pupils registered at the two collaborating schools. The consent forms will offer three participation options: 1. Only for sub-study 1; only for sub-studies 1 and 2; and for all four studies. This documentation will also be uploaded on the two schools’ online information platforms.
Second, an information meeting at the schools will provide football players and their parents/guardians with an opportunity to ask questions and talk to the research team about the project. Consent forms (as described above) will again be provided at this event. Players and their parents who agree to participate in the project can return the consent forms via their teachers (in an envelope), postal service or at the information evening.
Recruitment of coaches will also begin through the distribution of project information. We will hold a separate information event for coaches that will serve to answer their questions. Consent forms can be returned at the event, via postal service or the football academy.
Sample sizes
As outlined above, sub-study 2’s minimum sample size was calculated at 116. This number is based on previous studies’ statistics (
We aim to include six football players in total together with their coaches in sub-studies 3 and 4. Each player and coach will be treated as a case study (
In what follows, a description of each of the four sub-studies is provided. At the end, a summary of the analytic procedure is presented. Figure 2 visualizes the timeline of this research (Fig.
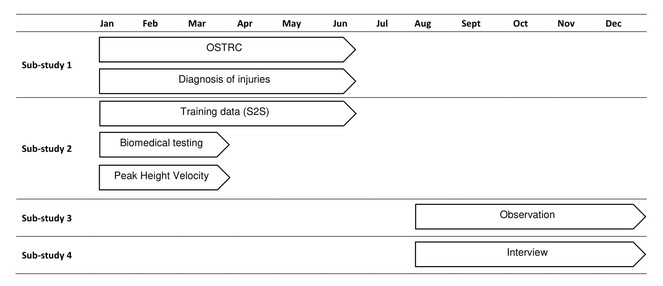
Sub-study 1 : Weekly from January – June 2018
The main purpose of sub-study 1 is to explore the occurrence, severity and types of injuries and health problems that Swedish youth football players experience. This sub-study will also test and validate the questionnaire we will employ for the Swedish youth football players.
Sub-study 1 contains three items:
- The adaptation and pilot testing of the OSTRC Questionnaire on Health Problems (
Clarsen et al. 2013 ). The questionnaire will be translated from English to Swedish and created through Gothenburg University's Sunet Survey Software. The questionnaire will then be tested in paper and electronically with Swedish children and youth to ensure that the questionnaire is child- and adolescent-friendly (i.e. language, user friendliness). The testing will focus on content (i.e. how do the children and youth understand the questions) and electronic operation on cell phones, tablets and a computer. - The completion of the adapted OSTRC Health Problems questionnaire. In January 2018, the recruited players will receive the survey with an email sent to their personal, parents' or school email addresses. Participants complete the survey from January to June 2018 on a weekly basis using their own or schools’ electronic devices. Reminder emails will automatically be sent if participants have not completed the survey.
- The medical diagnosis of indicated injuries. The participants that indicate an injury will be asked to visit their school’s medical staff or the collaborating football rehabilitation clinic, where the injury will be diagnosed and noted in the participants’ files. The injury diagnosis information will be passed on to the research team in encrypted form (only with survey code, not the player’s name).
Sub-study 2: Once in January/February 2018 and every week during January – June 2018
The main purpose of sub-study 2 is to investigate what combination(s) of biomechanical, clinical and training-specific patterns lead to the onset of injuries in Swedish youth football players.
Sub-study 2 contains two items:
Clinical and biomechanical testing of non-injured and healthy players who will visit the Center for Health and Performance (CHP) at the University of Gothenburg once during January/February 2018 and training protocol completed by coaches during January to June 2018.
The testing includes:
Clinical examination. Experienced staff members will carry out the clinical examination, which includes the measurement of range of motion (different planes and directions) for hip, knee, and ankle joints with the Mobee device (SportMed AG, Germany). All measurements will be performed bilaterally. The staff members will also document the incidence of past operations and overuse injuries, as well as other injuries to the lower extremities.
Isometric strength test. Isometric strength measurements for core and lower extremity muscles will be performed according to a standardized testing protocol. The following maximal isometric strength measurements will be tested: trunk extension, trunk flexion, trunk rotation, hip abduction, hip adduction, knee extension, and knee flexion. Calculations for the following strength balance ratios will be performed: trunk flexion:extension, trunk rotation right:left, hip abduction:adduction, knee extension left:right, knee flexion left:right, and knee flexion:extension. Each subject will perform two maximum isometric contractions at a standardized angle (
Running analysis. In the running analysis, all participants will run on a treadmill in the lab with a controlled speed of 10 km/h (SD 5%). Measurements will be recorded with the help of a 3D motion capture system (Qualisys AB, Göteborg, Sverige) consisting of sixteen infrared cameras at a sampling frequency of 400 Hz. Spherical markers will be attached on the skin at specific anatomical locations according to guidelines from the International Society of Biomechanics (ISB) (
Knee laxity. All athletes will perform a one leg squat to assess knee laxity (
Peak Height Velocity (PHV). By using the ‘maturity offset’ value, we can predict what age the child will achieve PHV (
Training protocol completed by coaches: January – June 2018
The coaches participating in the FIT project will document each training and match for each player in the training data program S2S – Secret to Sports (
Sub-study 3 and 4: Observations of sporting contexts and interviews: August – December 2018
The main purpose of sub-studies 3 and 4 is to examine sporting contexts, coaching practices, and norms in order to understand how contextual factors relate to injury development and prevention.
Observation. We will observe football contexts for a period of one month (or equivalent). Two training sessions per week and two competitions will be observed and we will produce field notes through voice records. An established observation schedule (
Semi-structured interviews. We will conduct interviews with each of the six observed athletes and coach(es). Each interview will be organized individually and will take approximately 60 minutes. Two established interview schedules, one for athletes (
Data management and analysis
Data from sub-studies 1 and 2 will be managed by saving them in separate excel documents. Data from sub-studies 3 and 4 will be transcribed into extended field notes and interview protocols. Data from testing of players will be saved per participant (with an identification number); data on training volume and intensity will be stored per team (from S2S program). Data from each of the four sub-studies will first be analyzed separately.
Data analysis. Quantitative analysis: Injury severity and injury location data will be presented using descriptive statistics. Categorical data will be presented in terms of frequency and proportion (%). Athletes will be divided according to injury severity or injury location. Injury incidence will be calculated by dividing the total number of injuries by exposure time and reported as rates per 1000 training and competition hours. Injury risk will be analyzed by utilizing log-binomial or log-Poisson regression analyses. Cumulative incidence of overuse injuries will be calculated using the Kaplan-Meier method to illustrate when overuse injuries occur during the season. Risk factors, such as biomechanical, clinical, and training-related or a combination of these, will be included in Cox proportional hazards regression analyses to identify early and late predictors of injury. A log-rank test will be used to compare the survival curves of risk factors. All calculations will be evaluated using SPSS statistics (Version 25, IBM Inc., Armonk, New York) and Mplus version 8 (
The qualitative analysis will be conducted along deductive thematic analysis principles (
Portfolio analysis. The results from the above individual analyses will be brought together in an integrated excel document. For those players that participate in all four sub-studies, portfolios of data will be created. These portfolios will contain analyzed quantitative and qualitative data, and annotations made by the research team. In order to perform an interdisciplinary analysis, the research team will discuss the integrated picture each portfolio generates. Through this process, we aim to produce multi-layered understanding of the factors involved in the development and prevention of injuries in youth football.
Relevance to society and research
With this study, we aim to affect organized youth sport at the local level, and in the long-term, Sweden-wide. The results from the different tests (sub-studies) will be given as individual reports to each football player, their coaches and parents/guardians. This will help to improve their sensitivity towards injury prevention and their knowledge about how to steer the training process from different perspectives in order to stay injury-free. After the final comprehensive evaluation of all sub-studies, guidelines for injury prevention in youth soccer will be developed and recommendations for how to manage a sustainable and long-term training process will be established. These guidelines will benefit sports as well as help sport organizations (also other sports besides football) and sport education institutions to optimize their (long-term) training planning and coach education. This will again affect athlete’s health in a positive way, and through this, their continued participation in sport and long-term physical activity. Life-long health can be promoted and medical costs reduced.
In relation to research, the project will provide evidence-based injury prevention recommendations (complex and interdisciplinary). This may close the earlier mentioned scientific gaps. The project will also develop scientific and research methodological guidelines, which can be tested in future prospective studies. The FIT project will also validate the OSTRC Questionnaire on Health Problems for children and youth, and showcase an interdisciplinary analysis procedure.
Funding program
PhD student fellowship from Swedish Research Council for Sport Science
Hosting institution
Department of Food and Nutrition, and Sport Science, University of Gothenburg
Ethics and security
Ethical approval was obtained from the regional ethical review board in Gothenburg on 18 October 2017 (Dnr 815-17).
Author contributions
NBR initiated and designed the FIT project with SG. SH led the drafting of the manuscript. AS, SG and NBR contributed to the writing. All authors read and revised the manuscript. All authors approved the final manuscript.
Conflicts of interest
No competing interests exist.
References
- No injuries, but plenty of pain? On the methodology for recording overuse symptoms in sports.British Journal of Sports Medicine43(13):966‑972. https://doi.org/10.1136/bjsm.2009.066936
- Olympism as education: analysing the learning experiences of elite athletes.Educational Review64(3):369‑384. https://doi.org/10.1080/00131911.2012.665846
- High performance sport and sustainability: a contradiction of terms?Reflective Practice15(1):1‑11. https://doi.org/10.1080/14623943.2013.868799
- Women's Artistic Gymnastics: An (Auto-)Ethnographic Journey.gesowip,Basel.
- Techno-rational knowing and phronesis: the professional practice of one middle-distance running coach.Reflective Practice15(1):53‑65. https://doi.org/10.1080/14623943.2013.868794
- Athlete learning in Olympic sport.Sports Coaching Review3(2):162‑178. https://doi.org/10.1080/21640629.2014.1059136
- Tracing the career paths of top-level women football coaches: turning points to understand and develop sport coaching careers.Sports Coaching Review3(2):117‑131. https://doi.org/10.1080/21640629.2015.1035859
- International Olympic Committee consensus statement on youth athletic development.British Journal of Sports Medicine49(13):843‑851. https://doi.org/10.1136/bjsports-2015-094962
- Risk factors for acute and overuse sport injuries in Swedish children 11 to 15 years old: What about resistance training with weights?Scandinavian Journal of Medicine & Science in Sports26(3):317‑323. https://doi.org/10.1111/sms.12432
- Are maturation, growth and lower extremity alignment associated with overuse injury in elite adolescent ballet dancers?Physical Therapy in Sport15(4):234‑241. https://doi.org/10.1016/j.ptsp.2013.12.014
- Using thematic analysis in psychology.Qualitative Research in Psychology3(2):77‑101. https://doi.org/10.1191/1478088706qp063oa
- Overuse Injuries, Overtraining, and Burnout in Child and Adolescent Athletes.PEDIATRICS119(6):1242‑1245. https://doi.org/10.1542/peds.2007-0887
- Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire.British Journal of Sports Medicine47(8):495‑502. https://doi.org/10.1136/bjsports-2012-091524
- The Oslo Sports Trauma Research Center questionnaire on health problems: a new approach to prospective monitoring of illness and injury in elite athletes.British Journal of Sports Medicine48(9):754‑760. https://doi.org/10.1136/bjsports-2012-092087
- Côtè J, Strachen L, Fraser-Thomas J (2008) Participation, personal development, and performance through youth sport. In: Holt NL (Ed.) Positive Youth Development Through Sport.13pp.
- Sport Injuries Aligned to Peak Height Velocity in Talented Pubertal Soccer Players.International Journal of Sports Medicine35(04):351‑355. https://doi.org/10.1055/s-0033-1349874
- Evaluation of Overuse Injuries in Children and Adolescents.Current Sports Medicine Reports9(6):372‑378. https://doi.org/10.1249/jsr.0b013e3181fdba58
- Physical Activity–Related Injury Profile in Children and Adolescents According to Their Age, Maturation, and Level of Sports Participation.Sports Health: A Multidisciplinary Approach9(2):118‑125. https://doi.org/10.1177/1941738116686964
- Five Misunderstandings About Case-Study Research.Qualitative Inquiry12(2):219‑245. https://doi.org/10.1177/1077800405284363
- Stopping sports injuries in kids.Current Opinion in Pediatrics24(1):64‑67. https://doi.org/10.1097/mop.0b013e32834ec618
- Understanding dropout and prolonged engagement in adolescent competitive sport.Psychology of Sport and Exercise9(5):645‑662. https://doi.org/10.1016/j.psychsport.2007.08.003
- A nine-test screening battery for athletes: a reliability study.Scandinavian Journal of Medicine & Science in Sports22(3):306‑315. https://doi.org/10.1111/j.1600-0838.2010.01267.x
- Consensus Statement on Injury Definitions and Data Collection Procedures in Studies of Football (Soccer) Injuries.Clinical Journal of Sport Medicine16(2):97‑106. https://doi.org/10.1097/00042752-200603000-00003
- Kinematic classification of iliotibial band syndrome in runners.Scandinavian Journal of Medicine & Science in Sports21(2):184‑189. https://doi.org/10.1111/j.1600-0838.2009.01045.x
- Risk factors for acute knee injury in female youth football.Knee Surgery, Sports Traumatology, Arthroscopy24(3):737‑746. https://doi.org/10.1007/s00167-015-3922-z
- Research in youth sports: Critical issues status.White Paper Summaries of Existing Literature
- Injury patterns in Swedish elite athletics: annual incidence, injury types and risk factors.British Journal of Sports Medicine47(15):941‑952. https://doi.org/10.1136/bjsports-2012-091651
- Sports-Specialized Intensive Training and the Risk of Injury in Young Athletes.The American Journal of Sports Medicine43(4):794‑801. https://doi.org/10.1177/0363546514567298
- Incidence of Football Injuries in Youth Players.The American Journal of Sports Medicine28:47‑50. https://doi.org/10.1177/28.suppl_5.s-47
- Injuries in youth amateur soccer and rugby players--comparison of incidence and characteristics.British Journal of Sports Medicine38(2):168‑172. https://doi.org/10.1136/bjsm.2002.003020
- Parents’ Reflections on their Child's Experiences of Emotionally Abusive Coaching Practices.Journal of Applied Sport Psychology24(2):191‑206. https://doi.org/10.1080/10413200.2011.608413
- Injuries in Youth Soccer.PEDIATRICS125(2):410‑414. https://doi.org/10.1542/peds.2009-3009
- Passion in Sport: On the Quality of the Coach–Athlete Relationship.Journal of Sport and Exercise Psychology30(5):541‑560. https://doi.org/10.1123/jsep.30.5.541
- Lang M (2010) Intensive Training in Youth Sports: A New Abuse of Power? In: Vanhoutte KK, Fairbairn G, Lang M (Eds) Bullying and the Abuse of Power.
- Maffulli N, Caine D (2005) The Epidemiology of Children?s Team Sports Injuries. Medicine and Sport Science. https://doi.org/10.1159/000085330
- Long-term health outcomes of youth sports injuries.British Journal of Sports Medicine44(1):21‑25. https://doi.org/10.1136/bjsm.2009.069526
- Maffulli N, Longo UG, Spiezia F, Denaro V (2010) Aetiology and Prevention of Injuries in Elite Young Athletes. Medicine and Sport Science. https://doi.org/10.1159/000321078
- Body pedagogies, coaching and culture: three Australian swimmers’ lived experiences.Physical Education & Sport Pedagogy18(3):317‑335. https://doi.org/10.1080/17408989.2012.666786
- Incidence, Severity, Aetiology and Prevention of Sports Injuries.Sports Medicine14(2):82‑99. https://doi.org/10.2165/00007256-199214020-00002
- Assessing Causation in Sport Injury.Clinical Journal of Sport Medicine4(3):166‑170. https://doi.org/10.1097/00042752-199407000-00004
- Sports injuries in children and adolescents.British Journal of Sports Medicine25(1):6‑9. https://doi.org/10.1136/bjsm.25.1.6
- An assessment of maturity from anthropometric measurements.Medicine & Science in Sports & Exercise34(4):689‑694. https://doi.org/10.1249/00005768-200204000-00020
- Strength of Isometric and Isokinetic Contractions.Physical Therapy60(4):412‑419. https://doi.org/10.1093/ptj/60.4.412
- Mplus User’s Guide.Eighth Edition.Muthén & Muthén,Los Angeles.
- Injuries and Associated Risk Factors Among Adolescent Elite Orienteerers: A 26-Week Prospective Registration Study.Journal of Athletic Training51(4):321‑328. https://doi.org/10.4085/1062-6050-51.5.01
- Multiple factors explain injury risk in adolescent elite athletes: Applying a biopsychosocial perspective.Scandinavian Journal of Medicine & Science in Sports27(12):2059‑2069. https://doi.org/10.1111/sms.12855
- Soccer injuries of youth.British Journal of Sports Medicine19(3):161‑164. https://doi.org/10.1136/bjsm.19.3.161
- Growth problems in youth elite sports. Social conditions, athletes’ experiences and sustainability consequences1.Reflective Practice15(1):78‑91. https://doi.org/10.1080/14623943.2013.868793
- "How Much Is Too Much?" The Social Construction of Elite Youth Athlete Exercise Tolerances From the Coaches' Perspective.Universitätsbibliothek Tübingenhttps://doi.org/10.15496/PUBLIKATION-6391
- Musculoskeletal Injuries in the Pediatric and Adolescent Athlete.Current Sports Medicine Reports4(6):329‑334. https://doi.org/10.1097/01.csmr.0000306295.49707.1f
- Subjective well-being and training load predict in-season injury and illness risk in female youth soccer players.British Journal of Sports Medicine51(3):194‑199. https://doi.org/10.1136/bjsports-2016-096584
- Psychology and socioculture affect injury risk, response, and recovery in high-intensity athletes: a consensus statement.Scandinavian Journal of Medicine & Science in Sports20:103‑111. https://doi.org/10.1111/j.1600-0838.2010.01195.x
- ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—part I: ankle, hip, and spine.Journal of Biomechanics35(4):543‑548. https://doi.org/10.1016/s0021-9290(01)00222-6
- Case study research: design and methods.Sage,London.